
“Quantum’s drive towards One Patient…One Record…and Total Connectivity’ achieves an important Intellectual Property achievement:
October 9, 2020, Lake Worth, Florida, USA – The Quantum Group, Inc. (“Quantum”) has received formal “Notice of Allowance” from the United States Patent and Trademark Office (USPTO) that the patent application US20180113980-A1 has successfully completed all reviews and is now in the process of being issued a document number, to be published on the USPTO website.
Titled: “System And Method For Making Patient Records Follow A Physician”
This new patent adds substantially to the robust portfolio of 20 issued patents and 19 pending patents. The patent enables an automated healthcare records system to assemble all the culminative information regarding the health of a patient and then directly associate this information and data with the patient. Presently, the digital electronic records (EMRs and EHRs) assign this information internally within the diverse programs creating major data silos that are difficult to penetrate due to HIPAA regulations and the substantially different data management system designs. Although this is a common practice among most EMR/EHR companies, it frustrates data exchange and proper data analysis as well as hampering integration between the various sources of data located on divergent EMR/EHR platforms.
SYSTEM AND METHOD FOR MAKING PATIENT RECORDS FOLLOW A PHYSICIAN
Abstract
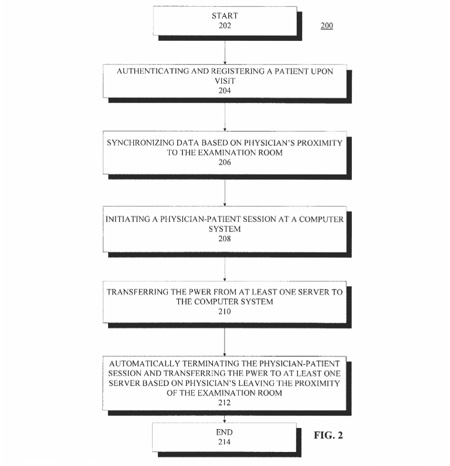
A system for providing access to patient records. The system can include computing devices and emitting devices carried by physicians for identifying each physician and scanning devices configured to detect and communicatively link to the emitting devices based on the proximity of the physician to an examination room, and a manager module communicatively linked to the scanning devices and configured to manage signal data from the scanning devices. The system can also include servers communicatively linked with the computing devices, scanning devices, and manager module, and configured to authenticate and register a patient, synchronize the physician identifier, patient identifier, personal wellness electronic record (PWeR), and examination room identifier based upon physician’s proximity to an examination room, initiate a session at the computing device at the examination room, transfer the PWeR to the computing device, and terminate the session based upon the physician leaving the examination room.
The patent application was originally filed December 3, 2009. It was challenged and we resubmitted it April 26, 2018 and is only now being awarded. Our diligence and persistence paid off as this is a CORE PATENT for us and the PWeR EHR platform as it provides a substantial differentiation of PWeR among competing EHR products and further aligns remarkably well with the national drive for interoperability and universal medical record.
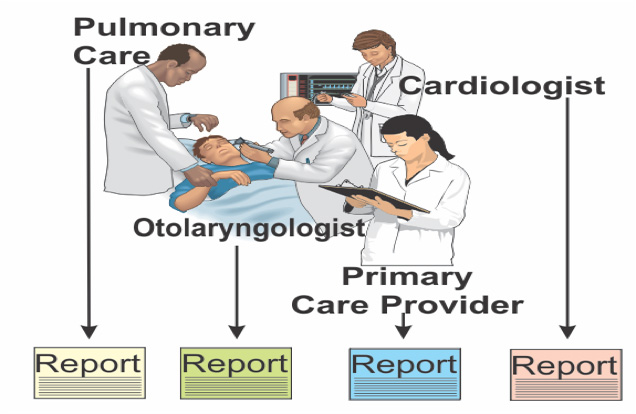
The Problem: Todays’ medical care often involves a team with specialized skills. Like the old joke of three blind men who examine an elephant, one describes an elephant as a trunk, the next as a tail, and the third sees an enormous foot. Each describes only what they examine and report on it. A complete picture requires the integration of the information by a primary care provider.
 Further, the examinations are not simultaneous as the picture suggests; they occur in diverse locations, at varying times and therefore the reports are seldom collected and exist at a single point. Typically, each provider stores their own data locally or at the best on a cloud server using a unique EHR. Even today, it is not uncommon to see a low-tech solution of a large file cabinet filled with paper records.
Further, the examinations are not simultaneous as the picture suggests; they occur in diverse locations, at varying times and therefore the reports are seldom collected and exist at a single point. Typically, each provider stores their own data locally or at the best on a cloud server using a unique EHR. Even today, it is not uncommon to see a low-tech solution of a large file cabinet filled with paper records.
Privacy laws, such as the 1996 Health Insurance Portability and Accountability Act (HIPAA) are often interpreted as requiring that individual patient health information remains private and portable. Net: the patient owns their own health data, not the providers; so why isn’t the data assembled around the patient, rather than the provider? That is the philosophy of PWeR: a health information system, that began its implementation not long after the HIPAA law was cast.
 Providers create, assemble, store, and protect the data, but it belongs to the patient. Nevertheless, providers are held legally responsible for maintaining the patient’s privacy rights under the law. Consequently, there is a natural desire to keep the patient records local and under the provider’s local control. The electronic health records system is intended to automate the full office system, yet forthe primary care provider in particular, it is difficult, if not impossible, to assemble all of the various records that pertain to one individual patient. One does not need to be a medical professional to see how intuitive and fundamental this is; however, the cost of obtaining, securing, managing and updating these patient records can consume or exceed the profit that a provider’s business can generate per patient.
Providers create, assemble, store, and protect the data, but it belongs to the patient. Nevertheless, providers are held legally responsible for maintaining the patient’s privacy rights under the law. Consequently, there is a natural desire to keep the patient records local and under the provider’s local control. The electronic health records system is intended to automate the full office system, yet forthe primary care provider in particular, it is difficult, if not impossible, to assemble all of the various records that pertain to one individual patient. One does not need to be a medical professional to see how intuitive and fundamental this is; however, the cost of obtaining, securing, managing and updating these patient records can consume or exceed the profit that a provider’s business can generate per patient.
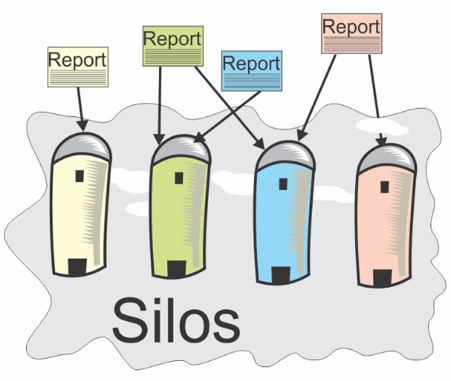 If every provider maintained just their own records, it would be like every farmer storing just their own crops in their own silos. That issue was eliminated a century ago, with common grain elevators for each agricultural region, and later giant vertically integrated agri-businesses that distributed food products and coordinated among the food providers.
If every provider maintained just their own records, it would be like every farmer storing just their own crops in their own silos. That issue was eliminated a century ago, with common grain elevators for each agricultural region, and later giant vertically integrated agri-businesses that distributed food products and coordinated among the food providers.
The analogous “Silo” problem in healthcare still exists and gets worse with increasing quantities of data is generated for each patient. Because many patients, particular those above 50 or with chronic ailments, work with multiple providers, the information in the data silos is often duplicated but not updated in all locations resulting in many of the records being obsolete and no more current than a patient’s last visit. The potential of bad data leading to bad decisions is significant. The adage of “two master’s is no Master” is poignantly true!
 One solution is to have the patient, or an advocate, collect and maintain the data from all the providers they visit, and to keep it current manually. This would require that they be constantly on the Internet and telephone collecting and communicating the latest patient data. It can be done; we even know of one patient who carried a file cabinet around as she required several providers, in different states, to cure her cancer. When the doctor would say: give me a week to collect your data and I will get back to you” or recommend a test or diagnostic exam she would say: “That’s not required, I have it right here”. That saved precious weeks and the cost of the follow-up visit with every provider. In the end, it saved enough time, that her fast-growing cancer was diagnosed and stopped in time to save her life. Multiply this scenario times 300 million people and it becomes obvious that only a computer, massively interconnected, with automated data collection can solve this coordination challenge on a national scale.
One solution is to have the patient, or an advocate, collect and maintain the data from all the providers they visit, and to keep it current manually. This would require that they be constantly on the Internet and telephone collecting and communicating the latest patient data. It can be done; we even know of one patient who carried a file cabinet around as she required several providers, in different states, to cure her cancer. When the doctor would say: give me a week to collect your data and I will get back to you” or recommend a test or diagnostic exam she would say: “That’s not required, I have it right here”. That saved precious weeks and the cost of the follow-up visit with every provider. In the end, it saved enough time, that her fast-growing cancer was diagnosed and stopped in time to save her life. Multiply this scenario times 300 million people and it becomes obvious that only a computer, massively interconnected, with automated data collection can solve this coordination challenge on a national scale.
An ideal system for managing health records would then collect data from multiple providers into a common database, where the patient’s files are assembled together in a common electronic health record, Of course, there are many more provider specializations, than this simple model. They are spatially diverse, and various providers each interact with the records at random times, occasionally at the same time. Yet, the records must maintain fidelity, organization and coherency of the data along with the highest levels of data security. Top down this must be an architecture that requires the Internet, massive servers, automated data collection, and incredible security to meet the demands of HIPAA. All this was envisioned in 2009 and implanted into a working model that evolved to the PWeR EHR system we have today.
In layman’s terms, the “Abstract” of the patent reads:
1: A system for providing access to patient records.
2: The system can include computing devices and emitting devices carried by physicians for identifying each physician and scanning devices configured to detect and communicatively link to the emitting devices based on the proximity of the physician to an examination room.
3: A manager module communicatively linked to the scanning devices and configured to manage signal data from the scanning devices.
4: The system can also include servers communicatively linked with the computing devices, scanning devices, and manager module configured to authenticate and register a patient, synchronize the physician and patient identifiers, Personal Wellness electronic Record (PWeR).
5: Examination room identifier based upon physician’s proximity to an examination room.
6: Autonomously initiate a session at the computing device in the identified examination room.
7: Transfer the PWER record to the computing device, and
8: Terminate the session, saving and securing all input based upon the physician leaving the examination room.
This what has been described above, translated from the ‘legalese’ and patent language.
The following flowchart defines the above process for controlling the provider’s office by way of the computer and select peripherals.
This is the “power” of PWeR®
Patents do not enable or give rights to production – they give the inventor the right to block others from implementing the novel concepts. This allowance adds a 21st patent to the portfolio. It protects investors by further providing IP value to trade with competitors in case of infringement. It will also yield a “freedom of action” for both engineering and marketing. Note: Two more patent allowances will soon be announced.

